

Background:Therapy related acute myeloid leukemia (t-AML) is a late complication following cytotoxic therapy for a primary neoplasm or a non-neoplastic disorder as autoimmune diseases and a highly fatal complication in patients treated for first primary malignancy. Therapy related AML are considered to have a worse prognosis and inferior outcome compared with de novo AML. The aim of this retrospective analysis is to describe clinical and biological characteristics and outcomes of these poor prognosis patients.
Methods:This retrospective analysis include 116 adult patients in 2 institutions (Leon Berard cancer center and Lyon Sud university hospital) between January 2006 and June 2019 treated with chemotherapy and/or radiation for different previous malignancies and who subsequently developed AML. We analyzed demographic characteristics, parameters related to previous malignancies (type, delay until occurrence of AML and treatment), to AML (cytogenetic and mutational profile, treatment and outcome). Event for overall survival (OS) was death and patients were censored at the date of last contact if alive or at the date of allogeneic HSCT. Event for disease free survival were death and first relapse.
Results:We analyzed retrospectively, 116 adult patients (57 male and 59 female) with median age of 67.5 [19 to 87] years diagnosed with t-AML according to 2016 revised WHO criteria and caused by exposure to chemotherapy and/or radiotherapy for previous solid tumors in 81 pts (70%) or hematologic malignancies in 35 pts (30%). Median time between diagnosis of previous neoplasm and AML was 5.4 [0.4-34.3] years. For the treatment of previous cancer, 48 pts (41%) received chemotherapy alone, 17 pts (15%) radiotherapy and 51 pts (44%) received both modalities. T-AML occurred after exposure to alkylating agents in 12 pts (12%), to agents targeting topoisomerase II in 7 pts (7%), to both agents in 65 pts (66%) and other treatment in 15 pts (15%). Cytogenetic profile was performed in 108 pts and was favorable in 4 pts (3.7%), intermediate in 46 pts (42.8%), unfavorable in 47 pts (43.5%) and assessment failed in 11 pts (10%). Eighty eight available leukemia samples were analyzed using molecular RT-PCR and, more recently, NGS profiling. Gene mutations concern 8 pts for FLT-3, 20 pts for Evi1, 1 pt for IDH1, 1 pt for IDH2 and 8 pts were TP53 mutated. Treatment of t-AML consisted in intensive chemotherapy (IC) in 59 pts (51%), hypomethylating agents (HMA) or low dose cytarabine in 29 pts (25%), best supportive care (BSC) in 28 pts (24%). Only 15 pts underwent allogeneic hematopoietic stem cell transplantation.
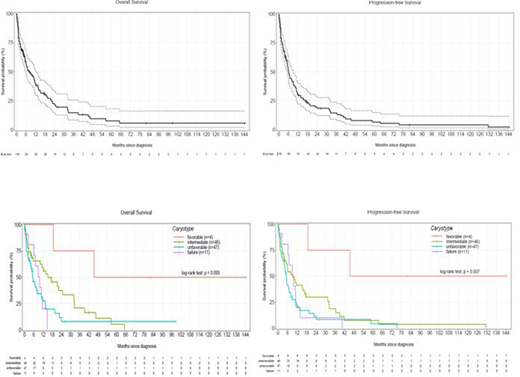
Median overall survival (OS) [95% CI] was 7.75 months [5.55-12.32] and median progression free survival (PFS) [95% CI] was 6.14 months [5.22-9.07] in whole cohort. According to cytogenetic risk group and as expected, the median survival is significantly longer in favorable than in intermediate and unfavorable risk group (45.3 vs 15.2 vs 5.4 mths for OS with p = 0.005 and 45.3 vs 10.3 vs 5.3 mths for PFS with p = 0.007).
Conclusion:This descriptive analysis confirm data of literature with poor prognosis and worse survival in unfavorable and intermediate risk groups of t-AML. However, pts with no comorbidities and candidate to IC had a significant better survival than those receiving HMA or BSC and should be considered for allogeneic transplantation
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal